In 2007, the St. Louis Fed summarized research about the 1918 influenza pandemic and used it to predict what would happen in a pandemic like the present covid-19 crisis. Their predictions have been pretty accurate. For example, the report predicted that low-income and minority households would have higher mortality rates than households with more resources. The report also made some predictions about the urban/rural divide:
• Given the positive correlation between population density and influenza mortalities, cities are likely to have greater mortality rates than rural areas. Compared with 1918, however, urban and rural areas are more connected today—this may decrease the difference in mortality rates between cities and rural areas. Similarly, a greater percentage of the U.S. population is now considered urban (about 80 percent) com-pared with the U.S. population at the time of the pandemic (51 percent in 1920)…
• Urban dwellers are likely to have, on average, better physical access to quality health care, though nearly 19 percent of the city population in the United States has no health coverage compared with only 14 percent of the rural population.28The question remains as to affordability of health care and whether free-service health-care providers, clinics and emergency rooms (the most likely choices for the uninsured) are able to handle victims of the pandemic.
The report warns about the need to “flatten the curve” to slow the rate of infection to prevent the healthcare system from becoming overwhelmed because, “Health care is irrelevant unless there are systems in place to ensure that an influenza pandemic will not knock out health-care provision”. This is much more important than it was in 1918 because of the dramatic improvements in the health care technology and epidemiology since 1918. In 1918, medical science didn’t even know that the pandemic was caused by a virus nor did they understand that it was spread by airborne droplets. It is amazing that even in 1918 the support of health care to take care of hydrating patients and keeping their body temperature in a safe range was extremely helpful. That was about all doctors were able to do in 1918 and the average household didn’t have the capability to do that kind of care well. The Fed report paints this picture of the limited ability of the healthcare system in 1918:
In 1918, the world was still engaged in World War I. Movement and mobilization of troops placed large numbers of people in close contact and living spaces were overcrowded. Health services were limited, and up to 30% of U.S. physicians were deployed to military service.3
In addition, medical technology and countermeasures at the time were limited or non-existent. No diagnostic tests existed at the time that could test for influenza infection. In fact, doctors didn’t know influenza viruses existed. Many health experts at the time thought the 1918 pandemic was caused by a bacterium called “Pfeiffer’s bacillus,” which is now known as Haemophilus influenzae.
Influenza vaccines did not exist at the time, and even antibiotics had not been developed yet. For example, penicillin was not discovered until 1928. Likewise, no flu antiviral drugs were available. Critical care measures, such as intensive care support and mechanical ventilation also were not available in 1918.4 Without these medical countermeasures and treatment capabilities, doctors were left with few treatment options…
In 1918, there was very little shared information about efforts to combat the flu so local officials couldn’t learn from the public health and medical efforts of other regions. World War I led to formal or informal censorship in most nations that would otherwise have had freedom of the press. In fact the disease misleadingly became known as the “Spanish Flu” simply because Spain happened to be a neutral country during the way and it was about the only nation with an unfettered press that was able to freely report about the unfolding disaster. The earliest known case of the pandemic was in Kansas and France was an earlier epicenter before it spread to Spain. Even though scholars are unclear about the origin of the flu, they agree that it did not begin in Spain and it was less severe in Spain than in many other areas. Because there was so little information sharing about the epidemic, nobody could learn from other nations about how to respond to the crisis and every local authority could only guess about what to do. For example, the Fed argues that, “complete quarantines worked (i.e., no activity allowed outside of the home) whereas partial quarantines, such as closing schools and churches but not public transportation or restaurants (as done in Philadelphia, St. Louis and Washington, D.C.) did little to stop the spread of influenza”, but the data gathering was primitive and even today there are uncertainties about what approaches worked best .
In the current crisis, public health experts have learned from experiences in other nations with social distancing and quarantine which has been more effective than most predicted. Although they failed to predict that social distancing would be so effective to combat the corona virus, this is partly because we have never had these kinds of public health measures in the history of the world and it is partly because science takes time to come to conclusions and we still don’t have enough data to understand what kinds of social distancing measures work best nor what vectors are most important in spreading the virus.
Despite the uncertainty, most experts in both public health and in economics agree that our shutdowns have been well worth it. The shutdowns worked a lot better than expected at reducing mortality so the advice of the experts worked out even better than most people would have hoped.
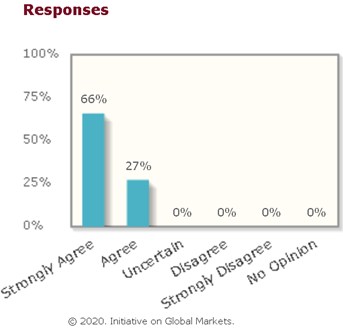
The University of Chicago’s business school regularly polls elite economists about a wide variety of topics and economists overwhelmingly agree that a lockdown is better for ‘the economy’ than letting the disease spread because the mortality and healthcare costs of a pandemic cause even more economic disruption than a voluntary lockdown. In effect, the fear and illness of widespread infections would cause the economy to shut down worse than what we have with deliberate stay-at-home strategies to slow the spread.
Abandoning severe lockdowns at a time when the likelihood of a resurgence in infections remains high will lead to greater total economic damage than sustaining the lockdowns to eliminate the resurgence risk.
For newer research that supports this conclusion, see Pandemics Depress the Economy, Public Health Interventions Do Not: Evidence from the 1918 Flu.
In addition to the economic effects, the mortality would be shocking. The pandemic would infect at least half of the world without social distancing efforts and even for people in their teens and twenties, the mortality rate is about 1 in 500.
That sounds small until you think about other comparable mortality risks in a given year. For example, would you be willing to go on a roller coaster ride that ‘only’ kills 1 in 500 riders? Most people would pay thousands of dollars to avoid being forced on such a ride and yet the corona virus is a lot less fun than a roller coaster. Even if you don’t die many more people get lung scarring and reduced lung capacity that is likely to be permanent.
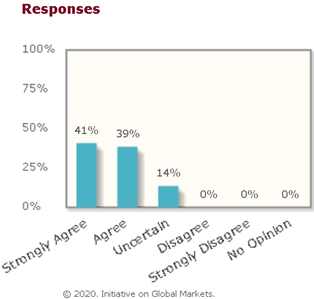
The University of Chicago’s poll also supported the idea that the government isn’t doing enough spending on testing, treatment, and searching for a cure:
Optimally, the government [should] invest more than it is currently doing in expanding treatment capacity through steps such as building temporary hospitals, accelerating testing, making more masks and ventilators, and providing financial incentives for the production of a successful vaccine.
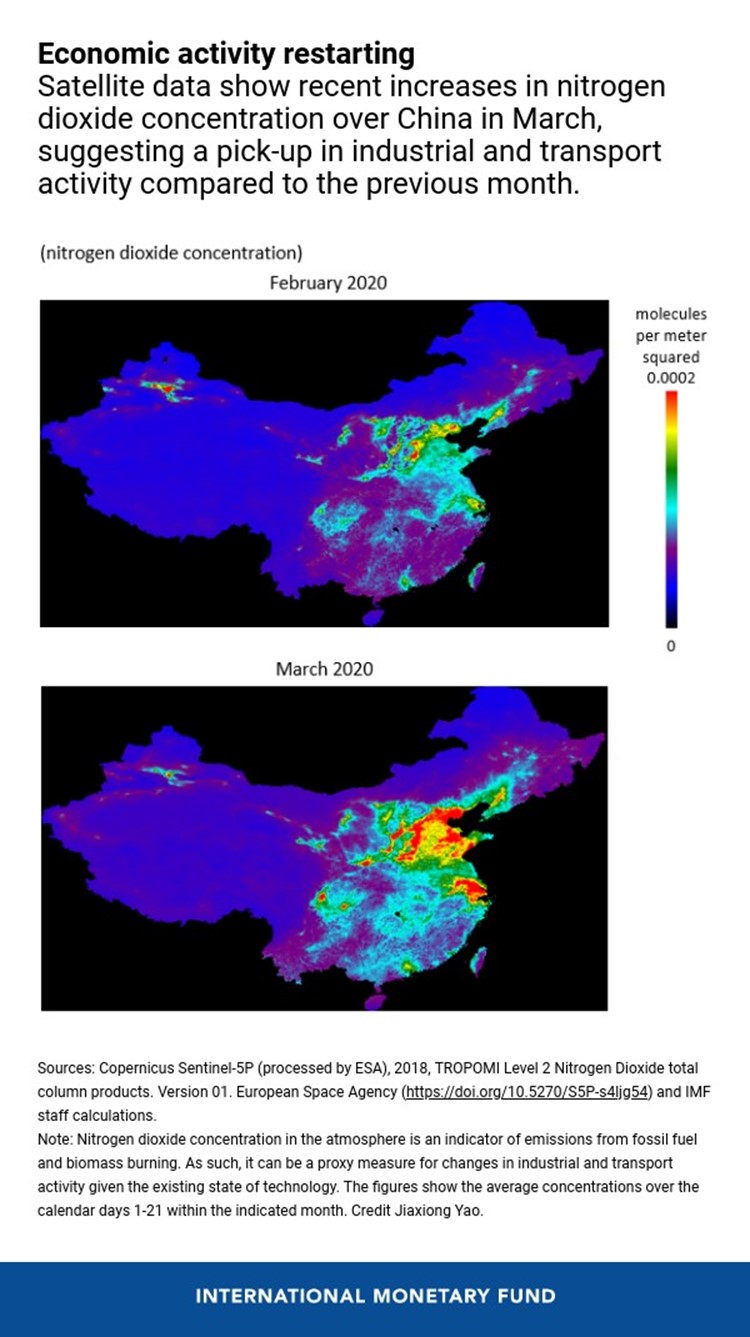
Another poll also showed that economists strongly agree that more testing is required before we can reopen the economy. This is what South Korea, Taiwan, Singapore, and China did. They used a massive testing program (relative to the total number of infections they had) to identify people who were sick and trace their contacts so that other people with possible infections could be identified and isolated until testing proved that they were virus free. As a result, these nations have been relatively successful at containing the outbreak and most of these nations avoided a lockdown. China has been successfully easing restrictions and restarting their economy as can be measured from satellite data showing a resurgence of air pollution as China’s industry restarts:
In order to get the economy back to work, America needs much greater investment in testing and contact tracing. There are many think-tanks and panels of experts who have come up with various plans for what it would take to successfully reopen the economy and they all agree that America needs to at least double our testing capacity (and get faster and more accurate at it) and we need to dramatically expand our public health infrastructure for tracing contacts for potential spread. That infrastructure has withered over the past decade and America is behind the Asian nations that have been more successful at limiting the spread of coronavirus without shutting down. Some states like Massachusetts are doing well at this, but to be successful, it needs to be a national effort. If any area of America lets down its guard, covid-19 will come roaring back and it will spread to the states that have been successful at keeping their own population safe. It is too hard to shut down state borders to prevent reinfection coming from out of state.
The consensus of The University of Chicago’s poll of elite economists is that the best way to stimulate the economy is a massive moonshot push to improve testing and tracing the coronavirus until we have a cure (or herd immunity) and we should be also investing massively in the effort to develop vaccines and/or treatments. Epidemiologists are divided about what percent of the population would need to get infected in order to achieve herd immunity, but most expect that at least 50% would need to get infected and that would result in millions of deaths, and worse economic disruption than our voluntary shutdown so it is a terrible option. There are a number of conspiracy theories circulating on social media about speculation that we have already achieved herd immunity because those conspiracy-theorists believe that the disease has an extremely low mortality rate and has already infected most people without them experiencing any symptoms. But that rumor is false. There is lots of evidence from random testing and from genetic studies that suggest that the percent of Americans who have been infected is closer to 1% than the 50%-80% required to achieve herd immunity.
Here is an estimate for European nations:

Long-term effects of the pandemic
There has been a lot of economic research about the effect of the black plague upon the economies of Europe, and the big conclusion is that it reduced inequality by reducing the labor supply when it killed “an astounding one-third to two-thirds of the population of Europe”. This caused wages to roughly double and rents to roughly drop in half and it reduced real interest rates. This radically reduced inequality except in places where elite property owners banded together to essentially enslave their workers by inventing serfdom in Russia and other parts of Eastern Europe to keep wages low.
I doubt the coronavirus pandemic will cause significant changes in the labor supply because modern public health measures will keep the mortality rate much lower than even the 1918 flu pandemic and unlike the 1918 pandemic which disproportionately killed the age group that was in their prime working years, this pandemic disproportionately kills retired people, so the demographic effect will be tiny and it will mostly just cause a small reduction in the dependency ratio by reducing the number of retired people the economy supports.













Leave a Comment