
The Nobel Prize for medicine went to cancer researchers this week who developed immunotherapy drugs that can be miraculously effective, but as Julia Belluz reports, the prize is also a reminder of how expensive the cancer treatments they developed have become:
Getting a cancer immunotherapy treatment costs more than a house in many cities in the US, more than putting a few kids through private college. The average cost of cancer drugs has increased from $50,000 per patient in the mid-1990s to $250,000 today. That’s four times the median US household annual income.
Immunotherapies in particular often cost more than $100,000 per patient. Doctors now use immunotherapies in combination, which means those costs can quickly double or triple. For some of the newest immunotherapies, the price tag is even steeper: When you include the value of the medical support necessary to deliver these treatments, a price tag of $850,000 per patient is not unheard of, according to Emanuel. “The drug companies say that they offer significant discounts to many patients, but because they won’t release this data, the list price is all that we have to go on,” he wrote.
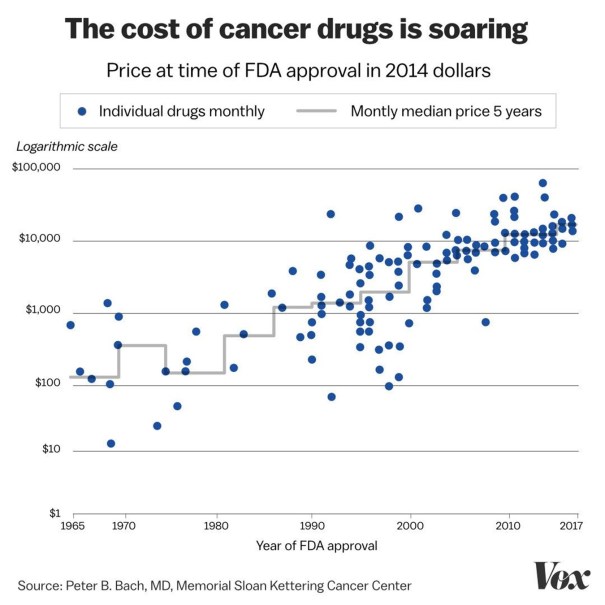
This chart from Peter Bach …says it all.
(Keep in mind that the y-axis here is logarithmic, not linear…) Patients with health insurance can be denied coverage for immunotherapies, even when it’s recommended by their oncologists.
The Washington Post reported on medical trials using a blood cancer drug called Imbruvica. Oncologists discovered that it was just as effective at lower doses than had been standard practice.
The researchers at the Value in Cancer Care Consortium, a nonprofit focused on cutting treatment costs for some of the most expensive drugs, set out to test whether the lower dose was just as effective — and could save patients money.
The researchers saw as a breakthrough because the pill had cost $148,000 per year. But when the manufacturers discovered the new research, they tripled the price per pill:
Within the next three months, the companies will stop making the original 140-milligram capsule, a spokeswoman confirmed. They will instead offer tablets in four strengths — each of which has the same flat price of about $400, or triple the original cost of the pill.
Just as scientific momentum was building to test the effectiveness of lower doses, the new pricing scheme ensures dose reductions won’t save patients money or erode companies’ revenue from selling the drug. In fact, patients who had been doing well on a low dose of the drug would now pay more for their treatment. Those who stay on the dose equivalent to three pills a day won’t see a change in price.
“That got us kind of p—ed off,” said Mark J. Ratain, an oncologist at the University of Chicago Medicine who wrote about the issue in the Cancer Letter, a publication read by oncologists. “We were just in the early stages of planning [a clinical trial] and getting it organized, and thinking about sample size and funding, and we caught wind of what the company was doing.”
Kevin Drum defended the pharmaceutical company, arguing:
what did these oncologists expect? Everyone knows that the price of drugs like Imbruvica doesn’t depend on the cost of actually manufacturing the stuff. Whether it costs a penny a pill or $100 a pill is irrelevant. These drugs are priced to recover their R&D costs based on the number of patients who are likely to use them. …there’s really no argument that the price of a cancer drug should decrease if it turns out you can use less of it. …The pharmaceutical company still has to recover its development costs, and that doesn’t change regardless of how big a dose is typically required.
This isn’t quite correct. First, and most importantly, a for-profit company never does pricing to recover R&D costs. Ever. R&D costs are sunk and for-profit companies price to maximize profits. R&D expenditures are irrelevant for determining pricing, but they are important for determining profit levels and that is important for determining whether a company goes bankrupt or not. But if a drug company goes bankrupt because it cannot repay the loans that financed R&D, then some other company will buy up the patent rights to sell the drugs if it can price the drug over the cost of manufacturing the stuff. That is the second part the Kevin Drum gets wrong. The manufacturing price always influence pricing because for-profit companies care about markup which is the price minus the marginal cost (manufacturing cost in this case). Suppose a company has been getting a $1000 markup, and the manufacturing cost was $200. If the manufacturing cost drops down to $100, the rational thing for a for-profit company to do is drop the price! The mathematical logic is hard to explain in words, but basically, if the profit-maximizing markup was $1000, then it doesn’t suddenly rise to $1100 simply because the manufacturing costs drop. The optimal markup is determined by the elasticity of the demand curve and unless demand is perfectly inelastic for some reason, the company can boost revenues by dropping the price and selling a higher quantity. Now, you could argue that the demand for drugs is very inelastic because people will die without them, but they aren’t perfectly inelastic or for profit companies would earn infinitely much money from selling them. So when for-profit companies get more efficient at manufacturing goods, they increase profits by reducing their selling prices.
Kevin Drum argues that setting the same price per patient regardless of the dosage makes the new pricing scheme fairer:
the new pricing model for Imbruvica may be fairer than the old one. Should a 300-pound person pay more than a 150-pound person just because their body requires a bigger dose? Should people with higher cancer loads pay more than those with lower cancer loads? That’s not at all clear, is it?
It is probably fairer to charge every patient approximately the same amount of money regardless of how much of the drug they acutally take because sicker or bigger patients generally don’t have more money. It is certainly more profitable to price this way. Although it might be fairer to patients, doctors don’t like the new pricing regime because it makes harder and more expensive to change dosages to respond to side effects and patient needs.
But the new regimen could undermine patient safety, Ratain and colleagues argue. People on Imbruvica often need to have their doses adjusted, because it can interact with other drugs. Physicians also may try lower doses when people have trouble tolerating the drug because of side effects, such as extreme joint pain.
The companies said in their statement that a dose exchange program with rapid shipment would allow physicians to make those changes. Under the old regimen, doctors could adjust the dose immediately by telling a patient to take one or two pills a day, instead of three, then return them to the higher dose when necessary. Under the new regimen, physicians will have to initiate a dose-switching protocol that requires paperwork. The phone number physicians have been given to call is only open Monday to Friday during business hours, several oncologists noted.
“I do share their concerns,” said Jennifer Brown, director of the Center for Chronic Lymphocytic Leukemia at the Dana-Farber Cancer Institute, who was not an author of the Cancer Letter paper. “We frequently change the dose of this drug, in relation to drug interactions in particular, and usually we need to do that basically instantaneously.”
Presumably the pills cannot be cut into smaller pieces for some reason or else everyone would just buy the maximum dose and cut the pills down to size. So every time a patient’s dosage is adjusted, another $148,000 set of pills must be bought and the unused pills returned for a refund. That is a lot of administrative expense.
The good thing about these outrageous prices is that they encourage more research to develop more therapies and more Nobel Prizes. The bad things about high prices is obvious to everyone. And prices are the highest in the USA. America accounts for less than 4.3% of the world population, but 45% of the world’s pharmaceutical expenditures in 2016! Americans use fewer drug prescriptions than many rich nations (Japan prescribed 60% more per person), but our prices are much higher which means that the USA provides the global pharmaceutical industry with much more than 45% of their profits. The US is also unusual in that nearly 75% of US drug expenditures went to branded drugs (as opposed to generics) even though 84% of prescriptions in the US specified cheap generics (the highest percent utilization of generics of any rich nation). So the US is paying the majority of the world’s pharmaceutical profits plus a tremendous amount of government-sponsored research in our state universities and grants to research hospitals and that buys a lot of Nobel Prizes.













Leave a Comment