Social spending is a ‘normal good‘ which means that richer countries (and richer people) spend more money on it. One of the odd facts about the United States is that we spend a lot more of our income on healthcare than any other country on earth, but we spend a lot less on other social services than most rich countries. Healthcare and other social spending are rarely added together, but healthcare is really a form of social spending. In fact, it is the biggest single category of social spending in most countries. In 2011, Elizabeth H. Bradley et al. (Benjamin R Elkins, Jeph Herrin, & Brian Elbel) published the first examination of how both forms of social spending add up to influence health outcomes and here is their graph. Notice that the US spends so much more on healthcare (the dark part of the line at the bottom), that even though the US spends less on other social spending, in total the US has larger than average combined social spending compared to most nations.
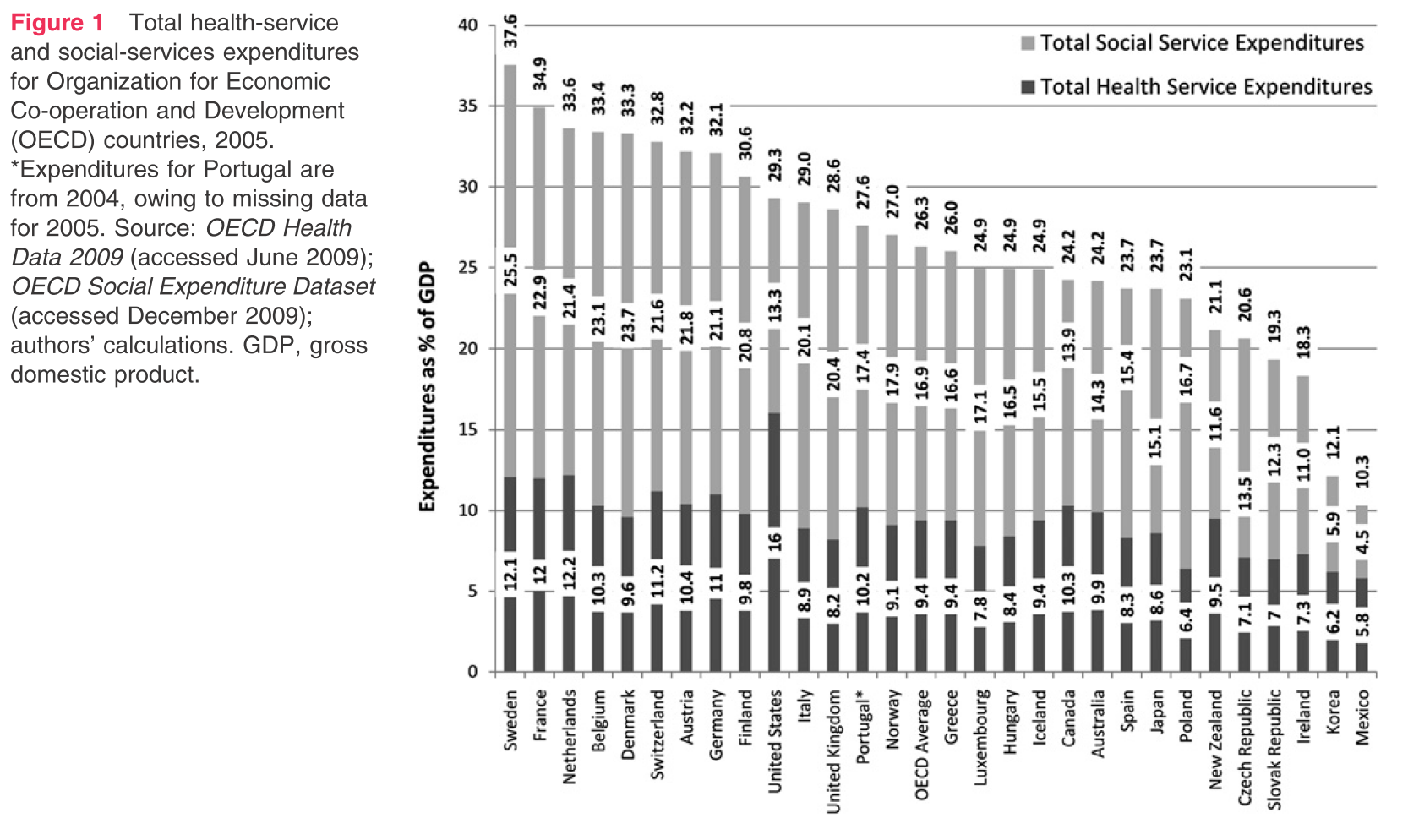
The US spends only 92 cents on non-health social services per dollar of healthcare spending whereas the average in other OECD nations is more than $2. Bradley et al. argue that countries like the US should divert more expenditures away from healthcare towards
…broader domains of social policy, such as unemployment, housing and education,… to accomplish the improvements in health envisioned by advocates of healthcare reform.
Elizabeth Bradley followed up by writing a book, The American Health Care Paradox, which was reviewed by Allan Joseph:
In terms of total spending that affects health, America’s actually right in the middle of the [OECD]—implying a gross misallocation of spending: too much spending in health services, and too little in social services. This is the core assertion of the book: implicating the social determinants of health as a central player in the problems of American healthcare.
Bradley and Taylor leverage this finding to create a quality book. They outline the historical development of the social-service and health-service sector, show that they split early in American history, unlike in other countries, which see them as two facets of the same system. That’s helpful information to have, if only to understand that the gulf between the two worlds is wide, and it’s not a simple task to shift spending from health services to social services.
…Take, for example, the story of Barry, a business executive whose startups went under:
As this business closed its doors in the same year it opened, Barry found himself financially and emotionally depleted. He was without a permanent home, unable to pay rent, and feeling like a failure…Barry is now morbidly obese, at six feet tall and 320 pounds, a binge eater, and prediabetic. He is uninsured and lives in temporary housing. He suffers from frequent leg cramps, periodic chest pain and despondency, and is in the early stages of developing some of the costliest disease to treat, including clinical depression, heart disease, and diabetes. (p. 53)
Barry was a healthy entrepreneur who risked all his money on a business and when the business failed, he found himself homeless and uninsured. His health rapidly deteriorated due to stress, poor diet, and depression. Many people like Barry wait to get medical help until a crisis forces them to go to an emergency room. Barry would undoubtedly qualify for Medicaid which could provide relatively inexpensive preventative care to treat his diabetes and heart disease, but it is not automatic, and many people in his situation do not find out that they qualify until a hospital emergency room signs them up after a health crisis.
A MillBank Quarterly investigation gave another case where social service spending was much cheaper than healthcare spending:
one organization learned that a woman in its care had visited the emergency room approximately 20 times in 1 month. The organization discovered that because she did not have transportation to her primary care doctor, she was using emergency services to meet her health needs. But when the team bought her a monthly bus ticket, her visits to the emergency room stopped. How many other people like her have similar transportation issues?
The woman had health insurance, but no transportation to get to her primary doctor. A monthly bus pass is MUCH cheaper and more effective than almost daily ER visits and it was cheaper for the hospital to buy her a bus pass than to keep providing almost daily ER services to treat crises that would be easily prevented. But even if the woman had no health insurance, it would still be cheaper to give her a bus pass and free outpatient checkups because Ronald Reagan created the legal entitlement that all people on American soil have a right to unlimited ER care at American hospitals. That entitlement makes it cheaper to end homelessness by providing free housing than to let homeless people clog our emergency rooms.
The paradox of American social service spending is that we will give millions of dollars to anyone (regardless of citizenship or ability to pay) who shows up to an emergency room in a health crisis, but we only give the dollars in the form of health spending. We are happy to spend millions of dollars on a high-tech premature birth for anyone, but once the baby is out of the hospital, we are less generous than most rich nations with helping all babies get good nutrition, shelter, daycare, and transportation to get vaccinations. Bradley et al. argue that stingy social spending helps explain why the US has higher infant and maternal mortality than other rich nations despite the US’s much greater expenditures on healthcare.
Low social spending also helps explain why the US has higher inequality than any other rich nation. Nobel laureate Angus Deaton wrote a famous work showing that middle-aged white Americans are dying earlier than in the past. Little of the reason is due to healthcare. It is mostly due to rising inequality which is creating more stress for white Americans than for minority groups whose recent history has seen bigger improvements relative to the lives of their parents.
Michael Marmot also has a new book, The Health Gap which makes a similar argument.
If you look at the probability that a 15-year-old will not survive to 60 in the US, it’s 13 percent. The US ranks 50th out of the 194 member countries of the World Health Organization on this measure, which means there are 49 other countries where a 15-year-old has a better survival chance than in the US. This is a country that spends far, far more on health care than any other country.
But this is not a health care issue. If you look at the causes of that premature mortality in the new study — it’s alcohol- and drug-related poisonings, suicide, other alcohol-related deaths, and external causes of death, and by that we mean homicide, violence, traffic pressures, and the like. So people don’t die of drug-related poisonings because of a lack of medical care; they die because they are taking drugs and/or committing suicide.
…The lower people are in the social hierarchy, the more likely they are to be obese, to be less physically active, to smoke, to suffer the consequences of alcohol. The social environment impacts on health by conditioning people’s behaviors. People under stress turn to alcohol, drugs, and violence because of that stress. It’s not very mysterious that people do that.
Marmot argues that reducing inequality will increase health. But reducing inequal access to healthcare would both reduce inequality and directly boost life expectancy by reducing the deaths that do result from inadequate healthcare.













Leave a Comment